Patient safety is defined as the freedom of a patient from unnecessary or potential harm associated with the provision of health care. A Harvard study by Prof Jha shows that 52 lakh medical errors (MEs) occur annually in India. According to the National Coordinating Council for Medication Error Reporting and Prevention (NCCMERP), a medication error is any preventable event that may cause or lead to inappropriate medication use or patient harm while the medication is in the control of the healthcare professional, patient, or consumer. Errors can occur throughout the medical use system. Medication error can occur at any of these stages: Prescribing, Ordering, Documenting, Transcribing, Dispensing, Administering, Monitoring. The NCCMERP taxonomy for medication errors defines four broad categories of errors: “No error”, “error- no harm”, “error- harm” and “error-death” (Aronson, 2009). Error prevention begins with the right practices to be followed: the right individual, medication, formulation, equipment, dose, time, route, documentation, storage and disposal (Sah et al, 2014). ME is one of the causes responsible for preventable mortality and morbidity (Ch’ng et al, 2021). Nursing plays a central role in medication management, except for prescribing. The discussion on patient safety came into light when the Institute of Medicine published its report, ‘To Err Is Human: Building a Safer Health System’ in 1999 (Sah et al, 2018). With the advancement of therapeutics in healthcare came multiple tests, procedures, techniques and drugs. Errors are inevitable, and hence making patient safety a priority is more important than ever. As per a cross-sectional study by Issacs et al (2021), the incidence of ME reporting is 57 percent.
According to a systematic review in 2020 by Baraiya et al, a nationalised medication error reporting system does not exist in India (Kashyap et al, 2020). Due to a lack of a reporting system and the absence of a data registration system, the accurate number of medication errors is difficult to trace (Baraiya & Kashyap, 2020; Cheragi et al, 2018).
The major factor for low rates of medication events is under-reporting. The fear of blame and penalty leads to underreporting. Reporting is important to thoroughly understand causes of errors, to prioritise opportunities for error prevention and to create long term environment for patient safe culture. Medication events can be used as a quality indicator. This study will improve our understanding of medication error types and contributing factors so that further prevention and control strategies can be implemented in a hospital setting.
Need for the study:
Medication error is the leading cause of concern and adverse outcomes the world over. Reporting helps to identify risks and minimise them in real life setting (WHO, 2024). Assessment of root causes aids in improving safety protocols and building a robust nursing standard. The study presented here adds more to the database by investigating the cause and its effects on patients as well, and also establishing a relationship between the cause to type of error.
Objectives
The study was set with following objectives:
1. To analyse the percentage distribution of medication errors across categories (prescribing, dispensing, administration, etc.).
2. To assess possible causes of error occurred.
3. To calculate the percentage of error that has resulted in an adverse event in a patient.
4. To assess types of corrective strategies implemented to prevent future medication errors.
Review of Literature
For this study, the literature search was conducted using PubMed, national and international nursing databases, and additional sources available on the internet. The terms used were medication errors, types, nursing, reporting, and preventive measures. The chi-square statistical test was utilised to analyse data. The current literature demonstrates the different types of medication errors and their causes. Many countries report having a centralised reporting system. The pivotal point here is that, although multiple safety protocols exist, medication error underreporting is still a matter of concern. Most studies tend to report the percentage of medication error, but very few dive into the steps taken into correction aspect and correlation.
Materials and Methods
The design of the study was cross-sectional, and observational. The study was conducted in a tertiary care hospital over one year.
Study population: Out of 125 subjects’ case files reviewed during the study period, 110 were identified as containing medication errors. All subject case files meeting this criterion were included in the analysis, representing a purposive sample based on the occurrence of medication error.
Data collection: Data was extracted from nursing and patient records of both genders, 18 years and above age group and from varied socioeconomic backgrounds. Data was collected as per a designed structured data collection form which included sociodemographic details, type of error, description of adverse event occurred, patient outcome (potential harm, death, etc.), contributing factors of the medication error, and intervention strategies implemented.
Variables: Type of errors, causes, adverse events, and preventive measures.
Procedure: All indoor patient file records of one year (1 May 2023 to 1 May 2024) were selected and scanned for medication error, type and its effect on the patient. Medication error was identified from incidence reporting reports, medication charts, nursing charts, clinical notes and prescriptions. Errors classified into categories (prescribing, transcription, administration, dispensing, documentation error, etc. Ethics: Approval was obtained from the Institutional Ethics Committee of the Maharashtra Medical Research Society (MMRS), Joshi Hospital, Pune (Maharashtra).
Analysis: Analysis was performed using Statistical Software for Social Sciences (SPSS) version 24 for MS Windows. SPSS was used for categorical data analysis (chi-square tests) to link error causes (SOP non-adherence, peak hours) with error types. Quantifying associations and significance, guiding targetted interventions, efficient data handling and output for clinical research. Chi-square test is suitable for testing statistical association between two categorical variables (such as a possible cause and different types of errors). Failing to adhere to standard operating procedures was the most common possible reason identified in this study; the statistical testing by correlating it with various types of errors gives us the opportunity to investigate the most common type of error potentially linked to this cause. Written informed consents were obtained from all patients and/or their legal guardians.
Results
A total of 125 participants were included in the study, of these 110 participants were identified with documentation-related medication errors (Table 1). The proportion of medication errors that directly affected patients was 0.9 percent (Table 2). Corrective measures primarily involved informing staff (57.3%), and educating staff (42.7%) (Table 3). Overall, 64.5 percent of medication errors were attributed to failure to comply with standard operating procedures (SOPs) (Table 4).
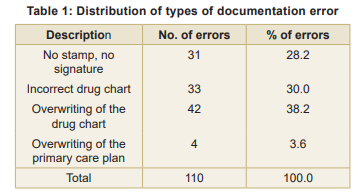
The distribution of types of documentation of errors (Table 1) shows that out of 110 total errors, the most common errors were related to overwriting of drug charts (38.2%, n=42), followed closely by incorrect drug charts (30.0%, n=33), and then errors involving no stamp or no signature (28.2%, n=31), while overwriting of primary care plans accounted for a smaller proportion (3.6%, n=4).
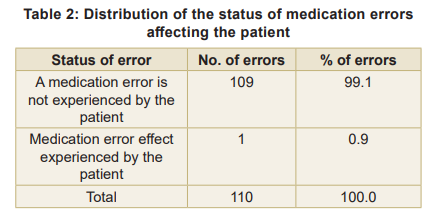
As evident from Table 2, the vast majority of medication errors (99.1%, n=109) were not experienced by the patients due to timely interventions, while only a small fraction (0.9%, n=1) of errors actually were experienced by the patients, indicating effective error mitigation measures in place. The effect of a medication error is summarised as potential to cause harm, no harm but requires monitoring, temporary harm requiring hospitalisation, near death event or death.
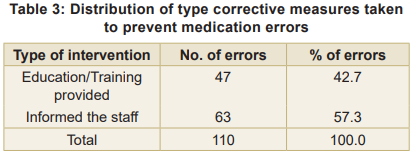
Table 3 reveals that the corrective measures taken to prevent errors were primarily focused on informing the staff (57.3%, n=63), while education or training was provided in response to 42.7 percent (n=47) of the errors, highlighting the importance of staff awareness and education in error correction.
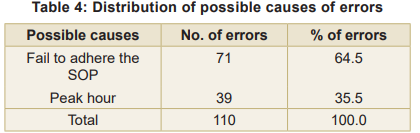
According to Table 4, the possible causes of errors were attributed to failure to adhere to Standard Operating Procedures (SOPs) in 64.5 percent (n=71) of cases, while 35.5 percent (n=39) of errors were linked to peak hour workload, suggesting that both process adherence and workload management are critical areas for improvement.
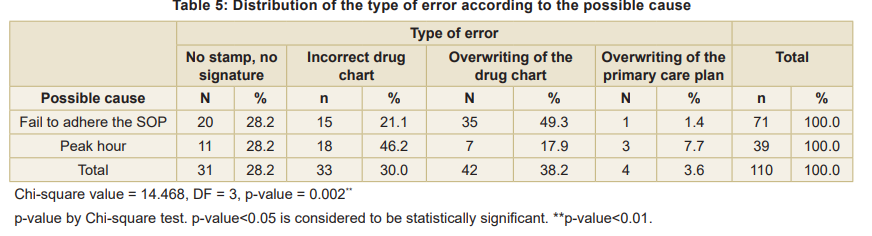
Documentation errors, such as overwriting of drug charts, absence of authentication, and incorrect chart entries, compromise the integrity of medical records and pose latent risks to patient care. The study analysed the distribution of types of errors (no stamp/no signature, incorrect drug chart, overwriting of drug chart, and overwriting of primary care plan) according to possible causes (failure to adhere to SOP and peak hour) (Table 5). A major contributing factor identified was non?adherence to standard operating procedures (SOPs), responsible for 64.5 percent of errors. This underscores the importance of reinforcing compliance with established protocols. Similar findings have been reported in previous studies, where deviations from SOPs were strongly associated with preventable medication errors (Isaacs et al, 2021). In addition, peak?hour workload emerged as a significant contextual factor, with incorrect drug charts being the most frequent error during busy periods. This suggests that cognitive overload and time pressure may impair nurses’ ability to maintain documentation accuracy. The statistically significant association between error type and cause (p = 0.002) further reinforces the need for tailored interventions that address both procedural adherence and contextual stressors.
Errors due to SOP non?adherence: The most frequent error was overwriting of drug charts (49.3%), followed by absence of stamp/signature (28.2%) and incorrect drug charts (21.1%). Errors during peak hours: The most frequent error was incorrect drug charts (46.2%), followed by absence of stamp/signature (28.2%) and overwriting of drug charts (17.9%). The chi?square test revealed a statistically significant association between the type of error and its possible cause (p = 0.002) (Table 5), indicating that error distribution varied significantly between causes such as non?adherence to SOPs and peak?hour workload. Documentation errors can delay treatment, obscure accountability, and increase the risk of adverse drug events. Therefore, fostering a culture of safety, encouraging transparent error reporting, and aligning practices with global initiatives such as the WHO’s ‘Medication Without Harm campaign’ are essential steps forward (WHO, 2016).
Conclusion
Overall, the results emphasise the importance of reinforcing SOP adherence, streamlining documentation practices, and implementing workload management strategies during peak hours. Strengthening these areas could significantly reduce documentation?related medication errors and enhance patient safety.
Nursing Implication
Strengthening Documentation Practices, regular audits of documentation can help identify recurring issues such as overwriting, missing signatures, and incorrect charting. Nurses should receive ongoing training and reminders about SOPs. Targetted education and feedback are essential for the prevention of events. Nursing supervisors should consider workload redistribution, staggered shifts, or additional staffing during high?volume periods to reduce cognitive overload and error risk. Encouraging nurses to report errors without fear of blame fosters transparency and learning.
Limitations
The single?hospital setting may limit generalizability to institutions with different workflows or documentation systems. Focusing on documentation errors restricts the broader view of medication errors. Absence of post?intervention analysis precluded assessment of long?term effectiveness.
Recommendation
Enhance and encourage electronic documentation, encourage SOP compliance, and promote continuous feedback. These recommendations bridge practice-level changes (nurse training, workload management) with system-level reforms (digital documentation, safety culture), ensuring a comprehensive approach to reducing medication errors.
References
1. MHFW, GOI. National Patient Safety Implementation Framework (2018-2025), April 2018, p 56
2. Aronson J.K. Medication errors: definitions and classification. Br J Clin Pharmacol 2009; 67(6): 599-04
3. Sah Aashita A, Khan ZH, Khokhar A. Basic concept of patient safety in healthcare delivery. International Journal of Current Research 2018; 10 (08):72926-32
4. Isaacs AN, Ch’ng K, Delhiwale N, Taylor K, Kent B, Raymond A. Hospital medication errors: A cross-sectional study. International Journal for Quality in Health Care 2021; 33(1). DOI - https://doi.org/10.1093/intqhc/mzaa136
5. Baraiya Komal, Thummar Kashyap. Medication error: A systematic review and comparison of reporting systems in the USA, UK and India. World Journal of Pharmacy and Pharmaceutical Sciences 2020; 9(8): 1011-30. 10.20959/ wjpps20208-16805
6. Cheragi MA, Manoocheri H, Mohammadnejad E, Ehsani SR. Types and causes of medication errors from nurse’s viewpoint. Iran J Nurs Midwifery Res 2013; 18(3): 228-33
7. WHO – Medication Without Harm Initiative, 2024 8. Medication Errors: Technical Series on Safer Primary Care. Geneva: World Health. Organization; 2016. Licence: CC BY-NC-SA 3.0 IGO
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.