Intensive Care Units (ICUs) are highly specialised settings where patients with life-threatening conditions are treated (Nates, 2016). These individuals often have a wide range of physical, psychological, spiritual, and social needs. ICU nurses must possess expert skills in assessing critically ill patients, identifying potential complications, delivering appropriate care, and collaborating effectively with the multidisciplinary critical care team (NANDA International). The nursing process is like a step-by-step, logical way for nurses to plan and guide everything they do when taking care of patients in a complete and personalised way. It’s a type of scientific thinking that requires nurses to use their sharp critical thinking skills to give clients the best possible care (Akolade et al, 2014; Ramakrishnan & Raja, 2008). The NANDA-I nursing diagnosis system, recognised globally, serves as a valuable framework for addressing patients’ overall needs and delivering personalised nursing care (Unai et al, 2015; Murar & Mehta, 2008). However, in intensive care settings, nursing practice is often hindered by limited understanding of the nursing process, insufficient patient assessment, and inaccurate formulation of nursing diagnoses (Korhan et al, 2014). Nursing diagnoses help to figure out what patients’ need and guide how their care is planned. By keeping track of nursing diagnoses, it can be better understood what patients need and ensure they receive the right care. Various researches revealed that nurses used nursing diagnoses from the domains 3, 4, 5, 11 and 12 for nursing assessment and care. It was observed that domains 7, 8, 9 and 13 were not commonly used for nursing assessment and care (akolade & Adejumo, 2014).
Objectives
This study was taken up to identify patients’ needs based on NANDA-I Taxonomy II among patients admitted in ICUs and to find out the correlation between patients’ needs in two different set-ups of ICUs. The hypothesis of the study tested was: There will be a correlation between patients’ needs as per selected domains of NANDA-I Taxonomy II in two different setups of ICUs.
Review of Literature
An extensive review of literature was done from various online journals retrieved from PubMed, ScienceDirect, Physiopedia, Research Gate, and other authentic websites. Review of literature done on various aspects, like NANDA-I, identified as a tool for effective nursing practice. Prolonged stay in the ICU increases the healthcare needs. ICU patients have a variety of unmet needs. Unmet needs in the ICU can worsen a patient’s existing medical condition and increase the length of ICU stay. The review of literature revealed that several studies have identified gaps in recognising and addressing various domains of patient needs, bringing to fore many unmet needs in the ICU. Effective utilisation of NANDA I nursing diagnoses has been shown to improve patient outcomes by identifying diverse care needs, facilitating individualised care, enhancing recovery, and reducing the length of stay in the ICU.
Materials and Methods
It was a cross sectional. descriptive study with 114 samples selected with consecutive sampling techniques from the Critical Care Unit and Anaesthesiology departments of a tertiary care hospital in Lucknow (UP), that met the inclusion criteria. This approach was practical and feasible in the ICU setting, minimising selection bias. It allowed for the systematic collection of data from a representative group of patients within the available timeframe.
Inclusion & exclusion criteria:
Length of stay > 48 hours, conscious patients sedated due to mechanical ventilation, patients undergoing haemodialysis, and haemodynamically unstable patients. Exclusion criteria: Pregnant mothers, patients with mental health ailments, head injury, patients with multiple organ failure and unconscious patients.
Tools used:
(i) Demographic profile - in this study, the common demographic profile includes age (in years), gender, distance from the health care setting, occupation, income, number of members in family, and availability of health care facility;
(ii) Self-structured 5-point Likert scale to assess patients’ needs based on NANDA-I Taxonomy II containing 92 items, constructed from the NANDA-I Taxonomy II Domains 1-7 and 9-12. Patients’ needs were categorised as more needs, moderate needs and less needs based on the 1/3rd of the total score.
Validity of tool:
Content and face validity were done. Validity was obtained from experts chosen among relevant and best clinical expertise in Medical, Nursing Faculties and Statisticians. Suggestions obtained from experts were incorporated in the final preparation of the tools.
Pilot study:
The pilot study was carried out on 12 samples after receiving ethical clearance. Administrative permission was taken from the Critical Care Unit, Departments of Anaesthesiology and Critical Care Medicine. The tool was found to be reliable and feasible. The reliability of the tool was found to be 0.722, calculated by Cronbach’s Alpha method.
Data collection procedure:
Data collection was done from December 2024 to January 2025. The researcher explained the information sheets, outlined the purpose and objectives of the study, and obtained written consent from participants. Then the participants were enrolled as per the inclusion criteria of the study. Data were collected using a self-structured Likert scale.
Informed consent:
Purpose of the study, study procedure, risks and benefits from the study, complications, compensation, confidentiality, and rights of participants were explained, and consent was obtained.
Results
As per Table 1:
l Domain 1 : Health promotion. Moderate needs were found among patients of the CCM department (72.13%) and the CCU & Anaesthesiology department (50.94%), with a significant correlation between both departments (p = 0.025).
l Domain 2 : Nutrition. It was observed that there were moderate needs found among patients of the CCM department (54.10%) and the CCU & Anaesthesiology department (41.51%), with significant correlation between both departments (p = 0.001).
l Domain 3: Elimination and exchange. Moderate needs were found among patients of CCM department (59.02 %) and CCU & Anaesthesiology department (56.60 %), with no significant correlation.
l Domain 4: Activity and rest. It was observed that there were moderate needs among patients of CCM department (44.26%) and CCU & Anaesthesiology department (49.06 %), with no significant correlatio.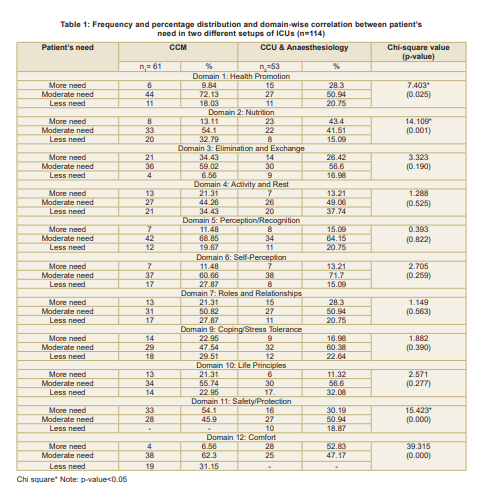
Domain 5: Perception/Recognition. It was observed that there were moderate needs among patients of CCM department (68.85%) and CCU & Anaesthesiology department (64.15%), with no significant correlation.
l Domain 6: Self-perception. Moderate needs found among patients of CCM department (60.66%) and CCU & Anaesthesiology department (71.70%), with no significant correlation.
l Domain 7: Roles and relationships. It was observed that there were moderate needs found among patients of CCM department (50.82 %) and CCU & Anaesthesiology department (50.94 %), with no significant correlation.
l Domain 9: Coping/Stress tolerance: It was observed that there were moderate needs found among patients of CCM department (47.54%) and CCU & Anaesthesiology department (60.38%), with no significant correlation.
l. Domain 10: Life principles. Moderate needs were found among patients of CCM department (55.74%) and CCU & Anaesthesiology department (56.60%), with no significant correlation.
l Domain 11: Safety/Protection. It was observed that there were more needs in the CCM department (54.1%) as compared to the CCU & Anaesthesiology department, with moderate needs (50.94%) followed by more needs (30.19%), with significant correlation (p = 0.000).
l Domain 12: Comfort. It was observed that there were moderate needs found among patients of CCM department (62.30%) as compared to CCU & Anaesthesiology department, with more needs (52.83%), with significant correlation (p = 0.000).
Discussion
Our findings indicate that moderate unmet needs are found in admitted ICU patients in various domains of NANDA-I, i.e., Health Promotion, Nutrition, Elimination and Exchange, Activity and Rest, Perception/Recognition, Selfperception, Roles and Relationships, Coping/ Stress Tolerance and Life principles in both departments. Results also show that more unmet needs were found in the domain Safety/ Protection among admitted patients of the CCM department, and moderate unmet needs were found in the CCU and Anaesthesiology department. Significant correlation was found in both departments in Domain Health promotion, Nutrition, Safety/Protection and Comfort. The above findings are supported by other studies. One study showed that the most frequently used nursing diagnoses by nurses were from domains 2, 3, 4, 5, 11 and 12 (Akolade & Adejumo, 2014). Another study revealed that the highest percentage of diagnoses was for the skin integrity impairment, impaired or mucous membrane, and the lowest number of diagnoses was impaired verbal communication. They demonstrated the need to focus on the patients as complete human beings, not only covering the biological aspects. Another study revealed that patients’ discomfort stemmed from both physical and psychological aspects, linked to their treatment, care, and the ICU environment. Notably, over half of the patients reported unmet needs during their ICU stay.
Recommendations
Use of NANDA nursing diagnosis for identifying the needs may reduce the cost of hospital stay by providing effective patient care in the ICU. The study may assist the student nurses in learning the appropriate utilisation of NANDA I in formulating nursing diagnoses and proceeding with an accurate nursing process. Each domain of NANDA nursing diagnosis may be applied independently to ensure greater precision and yield more comprehensive outcomes. The study recommends that it may be more fruitful when applied in various departments of the hospital with a larger sample size.
Limitations
i. Due to the limited timeframe, all the domains/ classes of NANDA nursing diagnosis were not included in the study.
ii. Data collection was time-consuming to cover all the domains of NANDA nursing diagnosis.
Conclusion
Patient needs identification among ICU patients based on NANDA nursing diagnosis helps to find out unidentified patients’ problems. Identification of the unmet needs of ICU patients can improve the planning of effective nursing care. Easy identification of unmet needs of the patients in ICUs by NANDA-I nursing diagnosis can assist the ICU nurses in the formulation of priority-wise nursing diagnoses and appropriate nursing care, which will enhance the quality of care. Easy identification of unmet needs of the patients in ICUs can assist the ICU nurses in the formulation of priority-wise nursing diagnoses and utilising various domains of NANDA I in providing quality care.
References
1. Nates JL. ICU Admissions and Discharge. 2016; 144(8): 1553-602. Available from: https://www.physiopedia.com
2. NANDA International. CC-BY-SA 4.0. June 2019. Available from: https://en.wikipedia.org/wiki/NANDA_International
3. Akolade FV, Adejumo OP. Nursing diagnosis domains utilised in the intensive care unit of a tertiary hospital in Ibadan, Nigeria. Int J Nurs Sci 2014; 43(2) PMID: 23474994. Available from: https:// pubmed.ncbi.nlm.nih.gov/25474994/
4. Ramakrishnan N, Jayaram Raja. Cost of intensive care in India. Rev Bras Ter Intensiva 2008 Apr-Jun; 12(2): 55–61. Available. from: http://www.bioline.org.br
5. Unai UA, Kostek O, Takir M, Caklili O, Uzunlulu M, Oguz A. Prognosis of patients in medical ICU. Northern Clinics of Istanbul 2015; 2(3): 189-95. PMID: 28058366. Available from: https://www.ncbi. nlm.nih.gov
6. Murar Y, Mehta S. ICU Care in India - Status and challenges. J Assoc Physicians India. May 2008 56: 221-22. Available from: https://www.researchgate.net
7. Gil BSN. The Nursing Process: A comprehensive guide. Nursing Fundamentals and Skills. Available from: https://www.nurseslab. com
8. Korhan AE, Yont G, Erdemir F, Müller-Staub M. Nursing diagnosis in intensive care unit. Crit Care Nurs Q 2014 Apr-Jun; 37(2): 219- 24. Available=from: https://pubmed.ncbi.nlm.nih.gov/24595259/
9. Ferreira AM, da Rocha EDN, Lopes CT, Bachion MM, Lopes JdeL, de Barros ALBL.Nursing diagnosis in intensive care: Cross mapping and NANDA-I taxonomy. Rev Bras Enferm 2015; 69(2): 307-15 Available from: https://dx.doi.org/10.1590/0034-7167.2016690214i
10. Oyama Y, Yamase H, Fujita K, Tashita H, Honda T, Yoshida K et al. Critically ill patients’ experiences of discomfort and comfort in the intensive care unit: A qualitative study. Aust Crit Care 2024; 38(6). Available from: https://www.researchgate.net/publication/384181175_Critically_ill_patients’_experiences_of_discomfort_and_comfort_in_the_intensive_care_unit_A_qualitative_descriptive_study
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.