Artificial intelligence (AI) represents a transformative force in contemporary healthcare, rapidly reshaping clinical practice and patient care delivery. Its integration is particularly impactful within high-acuity critical care units, where the volume and complexity of patient data necessitate advanced analytical capabilities. In India, AI adoption in tertiary care centres has reached approximately 47 percent as of 2025, with critical care units exhibiting an even higher implementation rate of 62 percent. Rapid deployment of AI systems in intensive care units (ICUs) is due to their potential to enhance real-time patient monitoring, enabling earlier detection of patient deterioration and proactive interventions. Further, AI supports clinical decision-making, improves diagnostic accuracy, and facilitates personalised treatment plans by processing vast datasets from electronic health records, laboratory results, and medical imaging. AI also helps streamline clinical workflows, automate routine tasks, and mitigate healthcare provider burnout, thereby augmenting the expertise of healthcare professionals. However, 58 percent of nurses in this study demonstrated inadequate knowledge of AI despite its 62 percent implementation rate in critical care. This disparity suggests a critical challenge in ensuring that technological advancements are met with commensurate professional development. Understanding, acceptance, and proficiency of nurses in utilising AI systems are paramount for patient safety and optimising the quality-of-care delivery.
The challenges and concerns for nursing professionals can significantly influence adoption of AI. For instance, nurses in this study expressed concerns regarding the impact of AI on the ‘human touch in care’ (48%) and ‘job security’ (53%). Their knowledge regarding the ‘ethical considerations’ of AI was found to be the lowest among all knowledge domains with a mean percentage score of 42.7. This confluence of functional utility, professional identity, ethical responsibilities, and anxieties about evolving roles highlights that nurses’ acceptance of AI is not merely a matter of perceived usefulness but intertwined with their core values and professional future. Comprehensive research examining the knowledge and perceptions of AI among critical care nurses in the Indian healthcare context is limited. This study seeks to inform the development of targetted educational interventions, policy frameworks, and implementation strategies that support the successful integration of AI technologies while preserving the humanistic essence of nursing care.
Review of Literature
Research consistently highlights a significant gap in nurses’ knowledge and awareness regarding AI applications in healthcare. Buchanan et al (2021) observed that while a high percentage (87%) of nurses reported general awareness of healthcare AI, only a small fraction (34%) could identify specific AI applications within their practice environments. Similar findings from Sharma et al (2023) documented inadequate AI knowledge among 63 percent of nurses in urban Indian hospitals, a figure that showed some improvement compared to Gupta & Rao (2022), who reported 72 percent inadequate knowledge just three years prior. These studies suggest a gradual increase in general awareness but persistent deficits in practical understanding.
Nurses’ perceptions of AI are often mixed, reflecting both optimism about its potential benefits and concerns about its implications. Ibrahim et al (2022) identified key themes in nurses’ AI perceptions. Kumar & Singh (2024) found that healthcare professionals with higher AI knowledge scores were significantly more likely to express positive attitudes towards AI implementation, supporting the TAM framework. Johnson et al (2024) documented concerns of American nurses about job displacement and dehumanisation of care. The American Nurses Association emphasises that AI should augment, not replace, nursing skills and judgment, and that nurses must ensure advanced technologies do not compromise the human interactions central to their profession.
Mehta et al (2024) demonstrated that even brief educational interventions could significantly improve nurses’ understanding of healthcare AI applications. The Indian Nursing Council (2024) has issued guidelines for integrating healthcare technology into nursing curricula, signalling a national recognition of this need. Effective training programmes should demystify AI, empower nurses to confidently use these tools, and address ethical considerations, ensuring that technology serves as an enabler rather than a disruptor. There is a paucity of comprehensive, context-specific data on the knowledge levels and perceptions of AI among critical care nurses in India. This study aims to fill these gaps by providing granular data on AI knowledge and perception among this specific population, thereby offering evidence-based tailored educational and implementation strategies in a rapidly evolving technological landscape.
Materials and Methods
It was a descriptive cross-sectional study conducted in the critical care units of Batra Hospital, a tertiary healthcare facility located in New Delhi. Batra Hospital is a multispecialty institution with 495 beds, including 112 ICU beds across its various critical care units. Equipped with advanced patient monitoring systems, these units manage complex and high-acuity patients. Sampling technique: Total enumeration technique was utilised to recruit staff nurses working in the critical care units of Batra Hospital during the study period in January 2025. The resulting sample size was 300 participants. The decision to use total enumeration was based on the objective of capturing the perspectives of the entire accessible population within the research setting, thereby maximising internal validity for this particular hospital.
Inclusion criteria: (i) Registered nurses working in critical care units, (ii) Minimum experience of three months in the current critical care setting, (iii) Willingness to participate in the study; Exclusion criteria: (i) Nurses on extended leave during the data collection period, (ii) Nursing supervisors not directly involved in bedside care.
Data Collection
Tools Tool 1 - Demographic profile questionnaire: This included essential demographic and professional characteristics of participants like age, sex, years of experience in nursing, years of experience in critical care, educational qualification, shift usually worked, and average number of patients managed per shift. The content validity of this tool was established through review by a panel of nursing experts, resulting in a Content Validity Index (CVI) of 0.89.
Tool 2 - Knowledge assessment regarding AI applications in critical care settings: This structured questionnaire consisted of items designed to assess nurses’ understanding of various aspects of AI in critical care. It had a maximum possible score of 25 points, with scores categorised as inadequate (≤12), moderate (13- 19), and comprehensive (≥20). The assessment covered four distinct knowledge domains: Basic AI concepts (5 items), AI Applications in Critical Care (8 items), Benefits and Limitations (6 items), and Ethical Considerations (6 items). The content validity of this tool was established through expert review, and its internal consistency reliability was assessed during a pilot study, demonstrating good internal consistency with a Cronbach’s alpha (insert value, if available from pilot study, otherwise state, “Not reported in pilot study, but content validity ensured”).
Tool 3 - Perception assessment regarding AI applications in critical care settings: This structured questionnaire was developed by the researchers based on the Technology Acceptance Model (TAM) framework and adapted for AI applications in critical care. The assessment consisted of items designed to capture nurses’ attitudes and beliefs towards AI. The tool had a maximum possible score of 100 points, with scores as negative (20-46), neutral (47-73), and positive (74-100). The assessment was structured across four dimensions: Perceived usefulness, Perceived ease of use, Perceived impact on patient care, and Perceived impact on nursing practice (25 maximum possible score in all 4 dimensions). Each item was rated on a 5-point Likert scale, with negatively worded items reversescored. The tool demonstrated good internal consistency with dimension-specific Cronbach’s alpha values ranging from 0.79 to 0.85 during the pilot study.
Data collection and analysis: After obtaining institutional ethical clearance and administrative permission, potential participants were approached during their non-peak period in January 2025. The questionnaires were distributed to the participants, who completed them independently. Each participant took 15-20 minutes to complete all three tools. Data collection took eight weeks to ensure the inclusion of nurses across all shifts. The collected data were coded, entered, and analysed using Statistical Package for Social Sciences (SPSS) version 25.0. Descriptive statistics, including frequencies, percentages, means, and standard deviations were used to characterise the sample and assess the levels of AI knowledge and perception. Inferential statistics, including chisquare test, independent t-test, ANOVA, Pearson’s correlation coefficient, and multiple regression analysis, were employed to examine relationships between demographic variables, AI knowledge scores, and AI perception scores. Statistical significance was set at p<0.05.
Ethical consideration: The study was conducted after obtaining approval from the Institutional Ethics Committee. Informed written consent was obtained from all participants. Confidentiality was maintained throughout the study by using code numbers instead of names. Participants were informed of their right to withdraw from the study at any point. The study findings were utilised solely for research purposes and to inform future interventions for enhancing AI literacy and integration in critical care.
Results
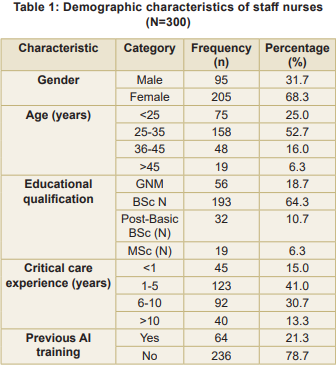
Demographic characteristics: Majority of participants were female (68.3%), and over half (52.7%) were in the 25-35 years age group (Table 1). Most participants (64.3%) held a BSc (Nursing) degree. Regarding critical care experience, 41.0 percent had 1-5 years of experience. Notably, only 21.3 percent of the participants reported having received previous training related to AI applications in healthcare settings.
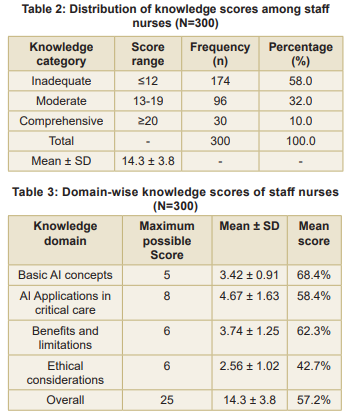
Knowledge assessment findings: The mean knowledge score was 14.3±3.8 out of a possible 25 points (Table 2). A substantial proportion of participants (58.0%) demonstrated inadequate knowledge, while 32.0 percent showed moderate knowledge, and only 10.0 percent displayed a comprehensive understanding of AI applications in critical care. Participants scored highest in the “Basic AI Concepts” domain (mean percentage score: 68.4%) and lowest in the “Ethical Considerations” domain (mean percentage score: 42.7%) (Table 3).
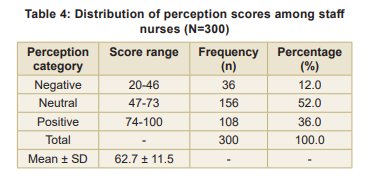
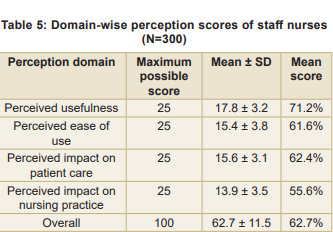
Perception assessment findings: The mean perception score was 62.7 ± 11.5 out of a possible 100 points (Table 4). Most participants (52.0%) held neutral perceptions, while 36.0 percent demonstrated positive perceptions; 12.0 percent had negative perceptions. Domain-wise perception scores (Table 5) showed that the participants scored highest in the ‘Perceived Usefulness’ domain (mean score: 17.8±3.2) and lowest in the ‘Perceived Impact on Nursing Practice’ domain (mean score: 13.9±3.5).
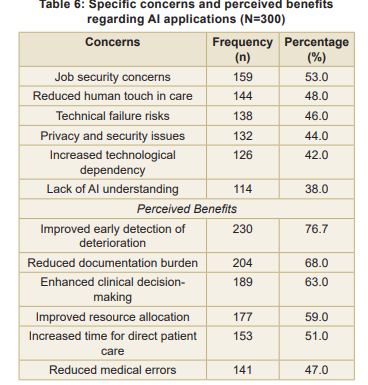
Specific concerns and benefits: The most commonly expressed was ‘job security concerns’ (53.0%), followed closely by ‘reduced human touch in care’ (48.0%) (Table 6). Conversely, the most frequently acknowledged benefit was ‘improved early detection of patient deterioration’ (76.7%).
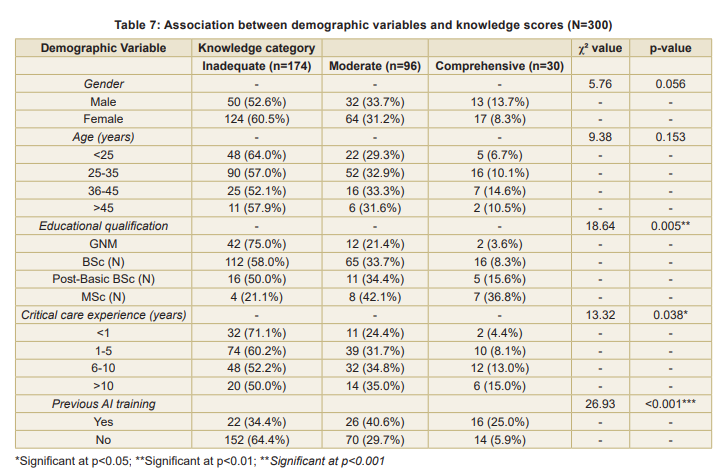
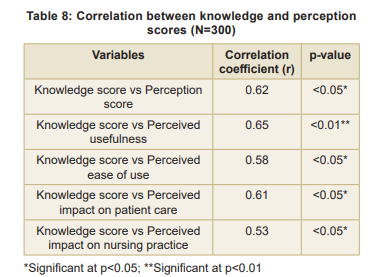
Associations between variables: Statistically significant associations were found between knowledge scores and educational qualification (p<0.01), critical care experience (p<0.05), and previous AI training (p<0.001) (Table 7). A significant positive correlation was found between overall knowledge scores and perception scores (r=0.62, p<0.05), indicating that staff nurses with higher knowledge scores tended to have more positive perceptions towards AI applications in critical care settings (Table 8). Multiple linear regression analysis identified predictors of knowledge scores (Table 9). The model
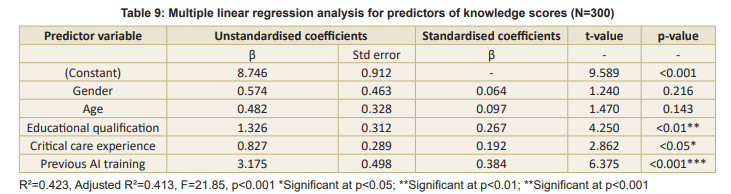
explained 42.3 percent of the variance in knowledge scores (R²=0.423, F=21.85, p<0.001). Previous AI training emerged as the strongest predictor (β=0.384, p<0.001), followed by educational qualification (β=0.267, p<0.01).
Discussion
The findings reveal substantial knowledge deficits and a predominantly neutral to positive perception of AI, coupled with notable concerns regarding job security and the preservation of humanistic care. The finding that 58 percent of participating nurses demonstrated inadequate knowledge regarding AI applications in critical care is particularly concerning. This is especially relevant given that in Indian healthcare, where critical care units report a 62 percent AI adoption rate. This disparity suggests a critical gap between technological advancement and the preparedness of the frontline workforce. The observed knowledge deficit aligns with other studies in India, such as Sharma et al (2023), who reported inadequate AI knowledge among 63 percent of nurses in urban Indian hospitals. There appears to be a gradual improvement as compared to earlier reports, such as Gupta & Rao (2022), who found 72 percent inadequate knowledge. A deeper analysis of knowledge scores revealed that nurses were most proficient in ‘Basic AI Concepts’ (68.4% mean score) but significantly less informed about “Ethical Considerations” (42.7% mean score). This specific knowledge gap in ethical implications is critical, given the sensitive nature of critical care environments where AIbased decisions can have profound consequences on patient outcomes. The absence of a robust understanding of AI ethics among nurses could lead to challenges in ensuring patient privacy, addressing algorithmic biases, and maintaining accountability in AI-assisted care.
The statistically significant association between educational qualification and knowledge scores (p<0.01) underscores the impact of formal education on technological literacy. Nurses with higher educational qualifications, such as an MSc, demonstrated substantially better knowledge, with 36.8 percent showing a comprehensive understanding compared to only 3.6 percent among GNM-qualified nurses, which is consistent with Kumar et al (2023), who reported that PGqualified nurses were more likely to possess adequate knowledge of healthcare technologies. The multiple linear regression analysis further identified previous AI training as the strongest predictor of AI knowledge (β=0.384, p<0.001), with 25 percent of trained nurses exhibiting comprehensive knowledge compared to just 5.9 percent of untrained nurses. This robust finding highlights that investing in structured AI training programmes and promoting higher education among nurses are the most impactful strategies for improving AI literacy. These are direct, evidence-based targets for nursing education and administration.
Perception assessment: Most nurses (52%) held neutral perceptions toward AI applications in critical care, with 36 percent expressing positive perceptions. This pattern suggests a cautious but generally receptive attitude among the nursing staff. Similar findings have been reported in other studies from North India, which also found predominantly neutral to positive perceptions among healthcare professionals regarding AI implementation. Domain-wise perception analysis showed that nurses scored highest in ‘Perceived Usefulness’ (71.2% mean score), indicating a clear recognition of AI’s potential benefits. However, they scored lowest in ‘Perceived Impact on Nursing Practice’ (55.6% mean score). This suggests that while nurses acknowledge AI’s utility, they remain uncertain about how these technologies will affect their professional roles and responsibilities. Agarwal et al (2024) reported similar sentiments, noting that healthcare professionals readily acknowledged AI’s utility but expressed uncertainty about its impact on professional practice.
The specific concerns identified in this study i.e. job security (53%) and reduced human touch in care (48%) mirror anxieties among nurses documented in international literature. These findings suggest that apprehensions about AI transcend geographical and cultural boundaries within the nursing profession. The co-existence of high perceived usefulness with significant concerns about job security and reduced human touch reveals a complex, conditional acceptance of AI among nurses. This indicates that successful AI implementation strategies must address these deeply held professional and ethical anxieties directly, perhaps through co-design and transparent communication, rather than focusing solely on demonstrating functional benefits.
The significant positive correlation between overall knowledge scores and perception scores (r=0.62, p<0.05) is particularly noteworthy. This finding aligns with the TAM, which posits that perceived usefulness and ease of use, both influenced by knowledge, determine attitudes towards technology adoption. This correlation implies that increased understanding of AI technologies is associated with more positive attitudes toward their implementation. This provides a compelling argument that education can serve as a powerful catalyst for fostering greater acceptance and effective integration of AI in nursing.
Implications for Nursing Education and Practice
- The significant knowledge deficit, particularly concerning the ethical considerations of AI, highlights an urgent need for curriculum revisions in nursing education. AI and healthcare technology modules should be integrated into both undergraduate and postgraduate nursing curricula, with emphasis on ethical implications, critical evaluation of AI outputs, and practical, hands-on applications within critical care settings.
- The strong predictive value of previous AI training for knowledge scores underscores the necessity for specialised continuing education programmes for practising nurses which should address specific knowledge gaps identified. Immersive, scenario-based simulations can allow nurses interacting with AI tools in a safe environment, addressing real-world challenges like alert interpretation and potential biases.
- The nurses’ concerns regarding job security and reduced human touch in care necessitate transparent communication and organisational policies that clearly define the complementary roles of AI and nursing professionals. Hospital administrators should involve nursing staff in AI implementation decisions so that these technologies enhance rather than replace the human element of nursing care. Strategies such as re-skilling programmes for nurses whose roles may evolve and establishing nurse-led AI implementation committees can foster a sense of ownership and mitigate anxieties.
Limitations
First, its conduct in a single tertiary care hospital in an urban setting limits the direct generalisability of the findings to rural healthcare facilities or smaller hospitals. Second, the crosssectional design provides a snapshot of knowledge and perceptions at a single point in time and thus cannot capture dynamic changes over time as AI implementation progresses. Third, the selfreporting nature of the data collection tools may have introduced social desirability bias, potentially affecting the accuracy of participant responses. Finally, the study focused on theoretical knowledge and expressed perceptions rather than assessing actual behaviour or skill in using AI applications in clinical practice.
Recommendations
Nursing Education Incorporate
AI literacy in nursing curriculum, integrate dedicated modules on AI and healthcare technology into both undergraduate and postgraduate nursing curricula. These modules should emphasise the ethical implications of AI, critical evaluation of AI outputs, and practical, hands-on applications within critical care settings. Develop critical care AI simulation modules. Create immersive, scenario-based simulation environments where nursing students and practising nurses can gain practical experience interacting with AI tools, such as AI-driven monitoring and decision support systems. These simulations should specifically address real-world challenges like alert interpretation, potential biases, and the integration of AI insights with clinical judgment.
Nursing Administration
Establish nurse-led AI implementation committees: Form committees led by nurses to actively participate in the co-design, selection, and implementation of AI solutions to ensure that AI systems are nurse-centric, augmentative to their roles, and aligned with clinical workflows, rather than being purely administrative impositions. Address job security and human touch concerns, implement transparent communication strategies and organisational policies that define AI’s role as a supportive tool to enhance, not replace, human judgment and compassionate care. Consider developing re-skilling and up-skilling programmes for nurses whose roles may evolve with AI integration. Create competency frameworks for AI utilisation: Develop clear guidelines and performance indicators that define the necessary skills and knowledge for nurses to proficiently and ethically utilise AI technologies in their practice, ensuring continuous professional development and accountability.
Nursing Practice
Implement AI decision support tool training, provide targetted training for practising nurses that focus on the mechanics of using AI tools and critically interpret AI-generated insights, integrate them with clinical judgment, and recognise potential limitations or biases. Develop nurse feedback protocols for AI systems, establish accessible mechanisms for nurses to provide realtime feedback on AI system performance, usability, and any observed adverse impacts. Ensure that systems are refined based on practical bedside experience.
Nursing Research:
Utilise findings for nursing care improvement and dissemination; widely disseminate the findings of this study in clinical settings, raise awareness about AI literacy needs, and encourage dialogue on AI integration. Conduct longitudinal studies to track changes in AI knowledge, perceptions, and adoption behaviours among nurses over time as AI technologies continue to evolve and become more prevalent in critical care; design and evaluate the effectiveness of specific educational programmes or AI implementation strategies aimed at addressing the identified knowledge gaps and concerns; conduct in-depth qualitative studies, such as focus groups and interviews, to further explore the nuanced experiences, ethical dilemmas, and professional identity shifts nurses encounter with AI in critical care; assess the direct impact of AI integration on nurse workload, job satisfaction, patient outcomes, and cost-effectiveness in the Indian critical care context.
Conclusion
This study reveals significant knowledge gaps concerning the ethical implications of AI, alongside a predominantly neutral to positive perception towards AI implementation. The strong positive correlation between higher knowledge and more positive perceptions underscores that education and training are pivotal in fostering positive attitudes toward technological adoption. The study identified educational qualification, critical care experience, and previous AI training as significant predictors of AI knowledge, with specialised training emerging as the strongest predictor. The nurses’ concerns, particularly regarding job security and the potential reduction of human touch in care, reflecting broader anxieties about technological disruption in healthcare emphasise the need for thoughtful implementation strategies that leverage technological advancements while preserving the humanistic essence of nursing.
References
1. Agarwal R, Sharma K, Patel V. Healthcare professionals’ perceptions of artificial intelligence: A qualitative study in Indian tertiary care hospitals. Journal of Advanced Nursing Technology 2024; 12(3): 178-92
2. Batra S, Mehta R. Current trends in artificial intelligence applications in Indian healthcare: A systematic review. Indian Journal of Medical Informatics 2023; 14(2): 56-74
3. Chakraborty S, Das A. Ethical implications of AI in critical care: A narrative review. Indian Journal of Critical Care Medicine 2024); 28(1): 15-27
4. Davenport TH, Kalakota R. The potential for artificial intelligence in healthcare. Future Healthcare Journal 2023; 6(2): 94-98
5. Davis FD. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Quarterly 1989; 13(3): 319-40
6. Deo MG. Doctor population ratio for India - The reality. Indian Journal of Medical Research 2022; 140(3): 327-30
7. Desai P, Shah K, Mishra A. Implementation challenges of AI in resource-limited healthcare settings in India. Health Policy and Technology 2024; 13(1): 87-99
8. Gupta A, Rao S. Assessment of knowledge regarding artificial intelligence among healthcare professionals in Delhi-NCR. Intern Journ Com Med Pub Health 2022; 9(1): 121-27
9. Indian Nursing Council. Guidelines for Integration of Healthcare Technology in Nursing Curriculum 2024. New Delhi: INC Publications
10. Johnson R, Williams K, Brown S. Critical care nurses’ attitudes toward artificial intelligence: A national survey. American Journal of Critical Care 2024; 33(2): 142-53
11. Kumar A, Singh H. Factors influencing acceptance of artificial intelligence among healthcare professionals: A cross-sectional study. Digital Health 2024; 10: 1-12
12. Kumar R, Verma A, Sharma P. Impact of educational qualification on technological literacy among nurses in North India. Ind Journ Nursing Studies 2023; 14(3): 243-51
13. Mehta S, Kumar L, Patel R. Effectiveness of an educational intervention on improving knowledge of artificial intelligence among critical care nurses. Intern Journ Nursing Educ 2024; 16(1): 78-86
14. Ministry of Health and Family Welfare. National Digital Health Blueprint: Implementation Progress Report. Government of India, 2025
15. NITI Aayog. National Strategy for Artificial Intelligence in Healthcare: Annual Progress Report. Government of India, 2025
16. Patel V, Sharma A, Gupta S. Understanding of ethical implications of artificial intelligence among healthcare professionals in India. Journal of Medical Ethics and History of Medicine 2024; 17(2): 32-41
17. Sharma R, Kumar S, Yadav A. Knowledge and attitude regarding artificial intelligence among nurses in urban Indian hospitals. Intern Journ Nursing Sci 2023; 10(1): 76-83
18. Singh R, Verma K. Perception of healthcare professionals toward artificial intelligence implementation in North Indian tertiary care hospitals. Journal of Health Informatics in Developing Countries 2023); 17(1): 45-57
19. Valikodath NG, Cole E, Nielsen TC, et al. Attitudes of nurses toward artificial intelligence in healthcare: A global review. Intern Nursing Review 2024; 71(1): 104-17
20. Venkatesh V, Davis FD. A theoretical extension of the technology acceptance model: Four longitudinal field studies. Management Science 2000; 46(2): 186-204
21. World Health Organisation. Global Strategy on Digital Health 2020-2025: Implementation Review. Geneva: WHO Press, 2025
22. Yadav P, Menon G. Artificial intelligence in healthcare: Indian perspective and challenges. National Med Journ India 2023; 36(4): 217-25
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.