Barbershops hold a significant place in Indian society, functioning not only as grooming centres but also as social and cultural hubs. Traditionally, barbers have played diverse roles beyond cutting hair and shaving; they have acted as confidants, messengers, and participants in community events such as weddings and rituals (Bizarre Culture, 2024). Many barbershops, particularly in rural and semi-urban areas, are modest establishments located along roadsides, in markets, or in public spaces (Salons Direct, 2018). These establishments are often family-run and have been passed down through generations. In urban areas, barbering has evolved, offering modern services like hair colouring, facials, and cosmetic grooming to meet changing trends and demands (Salons Direct, 2018).
out hygiene and infection control (Wazir et al, 2008). Barbershops involve close physical contact and the frequent use of sharp instruments, including razors, scissors, and clippers (Demisu Zenbaba et al, 2023). Inadequate sterilisation of tools, shared towels, and improper waste disposal can facilitate the spread of bacterial, fungal, and viral infections (Mandiracioglu A et al, 2009), including bloodborne diseases like Hepatitis B, Hepatitis C, and HIV (Cosmin 2023). Minor cuts or abrasions during grooming can increase the risk of infection (Incredible Indian barbers 2025). Many barbers, especially in informal sectors, lack training in hygienic practices (Bhatt A et al, 2022), often due to financial constraints or absence of regulatory guidelines (Roy S et al, 2021).
Need for the study
Barbering in India remains largely unregulated, with no mandatory training or standard operating procedures (SOPs) for infection prevention. This creates a public health risk, particularly in informal sectors where modern tools and techniques are introduced without adequate knowledge of hygiene (Quarm et al, 2021). The lack of structured training, absence of barber unions or associations, and minimal enforcement of safety standards further exacerbate the problem (Chand et al, 2022). Poor hygiene not only threatens client safety but also risks the livelihood and credibility of barbers (Mahmoud et al, 2021). Therefore, assessing their current knowledge and practices is essential to design targeted interventions, develop educational resources, and promote safer barbering practices to reduce disease transmission and protect community health (Al-Rabeei et al, 2021).
Objectives
The study was undertaken with following objectives.
1. To assess the knowledge and practice regarding infection preventive measures and hygiene among the hairdressers of Nadiad City.
2. To determine the correlation between knowledge and practice regarding infection preventive measures and hygiene.
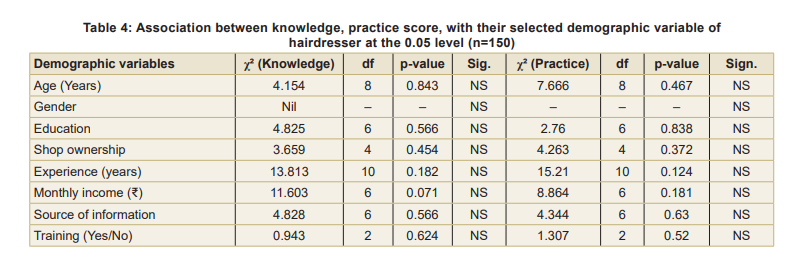
3. To examine the association between knowledge and practice scores with selected demographic variables among hairdressers.
Hypothesis
H1: There is no significant correlation between knowledge and practice regarding infection prevention and hygiene.
H2: There is no significant association between knowledge and practice scores and selected demographic variables.
Assumptions
1. Hairdressers may have poor to average knowledge and practice regarding infection prevention measures and hygiene.
2. The informational booklet will effectively enhance the knowledge and understanding of hairdressers regarding infection-preventive measures and hygiene practices.
Methodology
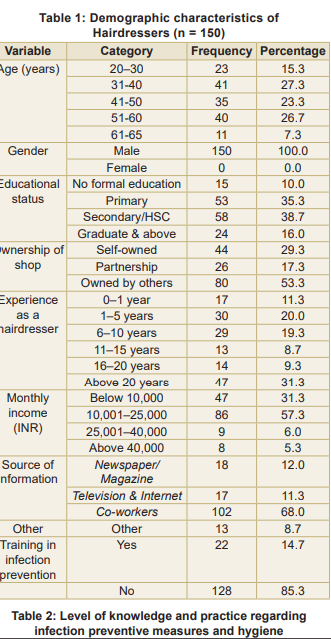
Study design and setting: A quantitative, cross-sectional survey design was employed to assess the knowledge and practices related to infection preventive measures and hygiene among hairdressers in Nadiad city (Gujarat). The study was conducted among 150 hairdressers selected from various barber shops across the city.
Eligibility criteria:
Participants were hairdressers aged 18-60 years with a minimum of three months’ work experience who voluntarily agreed to participate and provided written informed consent. Individuals who had undergone similar research study or basic hygiene and infection prevention training within six months before data collection, those who refused consent, or those with severe illness or chronic conditions that prevented participation, were excluded.
Sample size and sampling technique:
The estimated population of hairdresser shops in Nadiad City was approximately 200. A total of 150 participants were selected using proportionate sampling from all four zones to ensure fair representation, applying finite population correction for accurate coverage.
Formula: n = N / (1 + N (e²)
Where n is the required sample size, N is the total population (200), and e is the margin of error (set at 5% or 0.05). Substituting the values into the formula: n = 200 / (1 + 200 × 0.0025), n = 200 / (1 + 0.5), n = 200 / 1.5, n ≈ 133.33
The final sample size was set at 150, accounting for a 10 to 15 percent potential non-response rate, ensuring adequate representation, statistical validity, and reliable conclusions on hairdressers’ infection prevention practices. A stratified random sampling technique was used for this study to ensure equal representation of hairdressers from different areas of the city.
Data Collection Procedure
Before starting the study, the researchers obtained formal permission from the concerned authorities and took informed consent from each hairdresser who agreed to take part. All participants were clearly informed about the purpose of the study, their right to withdraw at any time, and the confidentiality of the information collected.
Data collection was carried out over a period of four months (January to April 2025) in Nadiad city. A total of 150 hairdressers were randomly selected from various parts of the city, including both roadside barbers and salon-based hairdressers.
Data were collected using a structured questionnaire and a 20-point observational checklist. The questionnaire covered demographics (age, gender, education, experience, and establishment type) and 20 multiple-choice knowledge questions on infection prevention and hygiene. Practices were directly observed during shop visits to minimize reporting bias. A master schedule ensured systematic data collection across four city zones. Tools were developed with expert input, reviewed by eight nursing professionals, and achieved excellent content validity (CVI: Demographics 0.89, Knowledge 0.87, Practice 0.89). Data were analysed and categorised as Poor, Average, or Good based on median scores. Ethical principles were strictly maintained.
Informational Booklet
Based on the study findings, a simple and easy-tounderstand informational booklet was developed to address the identified gaps in knowledge and practice among hairdressers. It aims to enhance their understanding and promote better infection prevention and hygiene practices in daily work. To ensure clarity and practical application, the booklet was prepared in the local language with clear illustrations, step-by-step guidelines, and practical tips for effective implementation.
Description of the Tool
The data collection tool was a structured instrument developed by the researchers to assess knowledge and practices regarding infection prevention and hygiene among hairdressers. It consisted of three sections:
Part I captured demographic details, including age, gender, education, work experience, and prior hygiene-related training. Part II comprised a 20-item multiple-choice knowledge questionnaire on personal hygiene, tool sterilisation, infection risks, and preventive measures, which was selfadministered by participants; and, Part III included a 20-point observational checklist used by the researcher during on-site visits to directly assess hygiene and infection control practices, minimising reporting bias. The tool was validated by eight nursing experts, yielding a Content Validity Index (CVI) of 0.89, indicating strong content validity. For better comprehension and applicability, it was prepared in the Gujarati language.
Ethical consideration:
Ethical clearance for the study was received from the Institutional Ethical Committee of Maganbhai Adenwala Mahagujarat University, Nadiad. Before data collection, formal permissions were obtained from the institution, shop owners, and individual participants. Informed consent was obtained after explaining the study’s objectives and procedures. Participant confidentiality was strictly maintained by using coded identifiers during data entry and analysis, ensuring confidentiality.
Results:
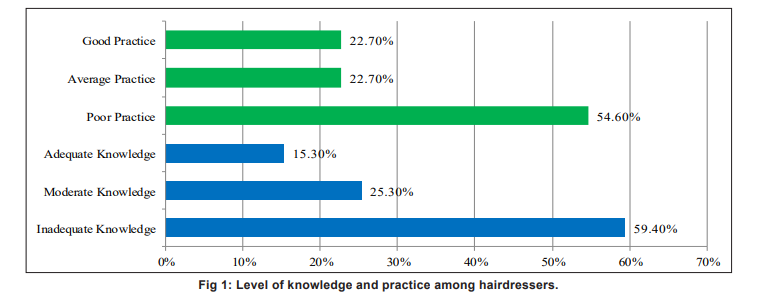
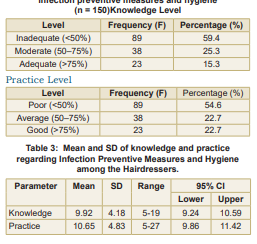
Table 1 (also Fig 1) show that a considerable number of hairdressers (59.4%) lacked knowledge, whereas 25.3 percent possessed moderate knowledge. Only 15.3 percent indicated good knowledge, indicating a significant gap in awareness of infection control and hygiene practices.
In terms of practices, 54.6 percent of participants displayed poor practice, 22.7 percent had moderate practice, and just 22.7 percent had good hygiene. This demonstrates that more than half of the hairdressers did not follow prescribed safety and infection control procedures (Table 2).
Table 3 shows that the mean knowledge score of hairdressers was 9.92 (SD = 4.18), and the mean practice score was 10.65 (SD = 4.83). The 95 percent confidence interval for knowledge ranged from 9.24 to 10.59, and for practice, it ranged from 9.86 to 11.42.
The calculated correlation coefficient (r = –0.067) indicates a weak negative correlation between knowledge and practice, which was found to be statistically non-significant (p = 0.412, df = 148) (Table 4). This suggests that there is no significant relationship between the knowledge and practice levels of the hairdressers in this
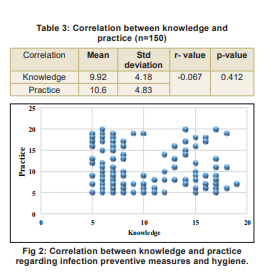
study. None of the demographic characteristics showed a statistically significant association with either knowledge or practice scores (p > 0.05 for all), highlighting the need for targeted educational interventions across all hairdresser groups to improve infection prevention awareness and hygiene practices (Table 4). Fig 2 depicts the correlation between knowledge and practice regarding infection preventive measures and hygiene.
Discussion
The present findings of this study reveal critical insights into the knowledge and practice related to infection prevention and hygiene among hairdressers in Nadiad city. The predominance of inadequate knowledge and poor hygiene practices among participants suggests a significant public health concern, especially in the context of services that involve close contact with clients and the potential for disease transmission. Interestingly, while the participants had a moderate mean knowledge score (9.92 ± 4.18), it did not.
Recommendations
The study identified a lack of standard operating procedures (SOPs) and the absence of a barber association in Nadiad city, leading to poor hygiene practices among hairdressers. To address this, an informational booklet was provided to enhance their knowledge and promote safe practices. It is recommended that the government develop and distribute clear SOPs on infection control specific to hairdressers. Establishing a local barber association could further support training and regulation. Regular workshops and health department visits should be conducted to reinforce hygiene practices and ensure long-term adherence, ultimately improving community health and safety standards.
Conclusion
The study revealed that the majority of hairdressers in Nadiad city had inadequate knowledge (59.3%) and poor practice (54.6%) regarding infection preventive measures and hygiene. The mean knowledge score was 9.92 (SD = 4.18) and the mean practice score was 10.64 (SD = 4.83), indicating low to moderate awareness and implementation levels. The correlation between knowledge and practice was positive (r = 0.67), but not statistically significant (p = 0.412). No significant association was found between knowledge or practice levels and demographic variables, such as age, education, experience, or prior training. These findings highlight a clear gap in knowledge and hygiene practices, emphasising the urgent need for structured training programmes to enhance infection control among hairdressers, regardless of their background or experience.
1. Clean Cut: A Profile of Barbers in India | Bizarre Culture. Bizarreculture.com. 2024 cited 2025 Apr 13. Available from: https://bizarreculture.com/clean-cut-a-profile-of-barbers-inindia/
2. The Importance of Hygiene in A Salon | Salons Direct, 2018. Available from: https://www.salonsdirect.com/blog/the-importance-of-hygiene-within-your-salon/
3. Wazir MS, Mehmood S, Ahmed A, Jadoon HR. Awareness among barbers about the health hazards associated with their profession. JAMC 2008; 20(2): 35-38. Available from: https://pubmed.ncbi.nlm.nih.gov/19385454/
4. Mandiracioglu A, Kose S, Gozaydin A, Turken M, Kuzucu L. Occupational health risks of barbers and coiffeurs in Izmir. Indian Journal of Occupational and Environmental Medicine 2009; 13(2): 92-96. Available from: https://dx.doi. org/10.4103%2F0019-5278.55128
5. Cosmin. Top Hygiene Tips for Barbershops: Ensuring a Clean and Safe Experience - Barbers and barbershops, online book appointments app, free for clients [Internet]. Barbers and barbershops, an online appointment app, is free for clients, May 2023. Available from: https://www. ringmybarber.com/top-hygiene-tips-for-barbershops-ensuring-a-clean-and-safe-experience/
6. Incredible Indian barbers-HWB, hairdressers without borders. 2016 [cited 2025 Apr 13]. Available from: https:// hwb-nonprofit.org/incredible-indian-barbers/
7. Bhatt A, Islam F, Shaikh A. Knowledge, attitude, and practices of barbers regarding blood-borne viral infections in the south-west district of Delhi. Indian Journal of Forensic and Community Medicine 2022; 9(4): 162-68. Available from: https://www.ijfcm.org/html-article/18096
8.Roy S, Dasgupta A, Bhattacharyya M, Paul B, Bandyopadhyay S, Pal A. Hazardous practices related to blood-borne viral infection transmission among male barbers: A study in a rural area of West Bengal. Indian Journal of Public Health 2021; 65(1): 22-27. Available from: https://journals.lww. com/ijph/fulltext/2021/65010/hazardous_practices_related_to_blood_borne_viral.5.aspx
9. Rajesh Manohara, Vishalakshmi M, Ramprasad S. Professional changes among the barbers: A study of Udupi Taluk. Journal of Emerging Technologies and Innovative Research 2023; 10 (6): 1810-17
10. Quarm MD, Mthembu J, Zuma K, Tarkang EE. Knowledge, attitudes and prevention practices regarding HIV/AIDS among barbers in Ho municipality, Ghana. Journal of Social Aspects of HIV/AIDS. 2021 Jan 1; 18(1): 42-51. Available from: https://pubmed.ncbi.nlm.nih.gov/33641600/
11. Chand D, Mohammadnezhad M, Khan S. Levels and predictors of knowledge, attitude, and practice regarding the health hazards associated with barber’s profession in Fiji. INQUIRY: The Journal of Health Care Organisation, Provision, and Financing 2022 Jan; 59: 004695802211001
12. Mahmoud S, Awadin L, Hassan A. Occupational Health Risks of Barbers: Knowledge, practices, and self-reported symptoms. Egyptian Journal of Health Care 2021; 12(2): 1562-82. Available from: https://ejhc.journals.ekb.eg/article_199657_47941c1aed6e6bbd44f5404aca077e87.pdf
13. Al-Rabeei NA, Al-Thaifani AA, Dallak AM. Knowledge, attitudes and practices of barbers regarding hepatitis B and C viral infection in Sana’a city, Yemen. Journal of Community Health. 2011 Dec 25; 37(5): 935-39
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.