B lood pressure is an essential vital sign and refers to the pressure exerted by the blood on the walls of arteries when the heart pumps it (NCI, 2011), which can be measured invasively and non-invasively. The non-invasive method of blood pressure (BP) measurement requires the use of a sphygmomanometer, which is a blood pressure monitoring device, composed of an inflatable cuff to collapse and then release the artery under the cuff in a controlled manner. There are various types of sphygmomanometers, but this comparative study focused on comparing the readings of aneroid and digital sphygmomanometers on patients admitted in male and female medical and surgical units of Nehru Hospital in PGIMER, Chandigarh.
Need for the Study
A comprehensive study in UK examined the comparability of measurement precision of all the three types of sphygmomanometers and found that the accuracy of digital instruments is almost equal to mercury instruments, while higher failure rate existed with the aneroid ones. Hence, the authors recommended the use of inexpensive and easy to use digital instruments by general practitioner during home visits. However, such evidence is sparse in the Indian context, and there is an clear need for more feasible and inexpensive instruments because of the enormous population size, low economic status of people and less tendency to seek institution-based medical care (Mion & Pierin, 1988). It was estimated that a rise in systolic BP of only 5 mmHg would result in a 25 percent increase in the chances of fatal stroke and fatal myocardial infarction while findings also substantiate the catastrophic consequences of underestimating blood pressure would result in inappropriate treatment with antihypertensive medication that will badly impact the health of Indian population (Shahbabu et al, 2016). So, the authors planned the study to compare variations in BP measurements with aneroid and digital sphygmomanometers.
Hypothesis
Ho : There will be no significant variations in the BP measurements by aneroid sphygmomanometer and digital sphygmomanometer at the 0.05 level of significance. H1: There will be significant variations in the BP measurements by aneroid sphygmomanometer and digital sphygmomanometer at the 0.05 level of significance.
Objectives
The study was set with following objectives: (a) To assess the socio-demographic and clinical profile of study participants. (b) To accept the null hypothesis. (c) To compare the blood pressure readings measured by aneroid sphygmomanometer and digital sphygmomanometer among patients admitted in selected wards of Nehru Hospital, PGI Chandigarh.
Review of Literature
Dasgupta et al (2021) conducted a cross-sectional research study on 400 participants, which was selected through a systematic random sampling technique from the OPD. The calculated Cohen’s Kappa value of 0.59 showed moderate agreement in the diagnosis of hypertension by both instruments, and there is obvious dissent between SBP and disagreement between diastolic blood pressure (DBP) of aneroid and digital sphygmomanometer as calculated through bland Bland-Altman plot. Shekhar et al (2020) carried out a comparative study of blood pressure recording from a conventional mercury sphygmomanometer, and from Android and digital devices with 102 participants. The results showed that the readings are comparable and can be used in practice. Chandrashekhar et al (2021) conducted a comparative study of mercury sphygmomanometers and automated BP measurement machines with a randomised sample of 224 patients. The study concluded that there was no significant difference in recorded values between mercury sphygmomanometers and automated digital sphygmomanometers (Rizfan et al, 2023). A study was conducted to check the accuracy of automated cuff blood pressure monitors in a special population, which led to a result that although the mercury sphygmomanometer can be replaced by a digital sphygmomanometer in clinical settings but there are some instances where the mercury sphygmomanometer remains a gold standard (Stergiou et al, 2023).
Methodology
This is a comparative study. Using the total enumeration technique, 300 patients aged above 18 years admitted in medicine and surgical units of a tertiary care hospital were enrolled. Blood pressure of each patient was measured using the same arm by well-calibrated, standardised aneroid and digital sphygmomanometers for all the participants. Three blood pressure measurements were obtained, each by an aneroid and digital sphygmomanometer at an interval of 3 minutes between each measurement. A pause period of 10 minutes was given between measurements by the two devices. The study protocol was approved by the Institute’s Ethics Committee.
Results
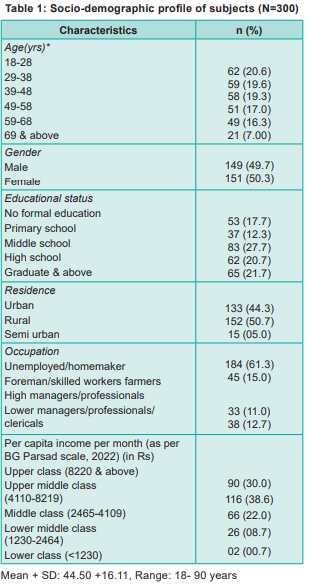
Socio-demographic profile of subjects Table 1 shows the socio-demographic profile of subjects. The mean age, standard deviation (SD)of the subjects was 44.50 + 16.11 years with a range of 18-90 years. About 21 percent of subjects were between the ages 18-28 years. About half the subjects (50.3%) were females and (remaining 49.7%) were males. Around 28 percent of the subjects were educated up to middle school level, while 12.3 percent had acquired primary school level education. Half of the subjects (50.7%) were residing in rural areas; urban population comprised 44.3 percent of the subjects, and the remaining (5%) were residing in semi-urban areas. As for occupation, a maximum number of subjects (61.3%) were unemployed/homemakers, while only 11 percent were managers/professionals. Around 39 percent had the socio-economic status of upper middle class, and the lower class was formed by the least number of subjects (0.7%).
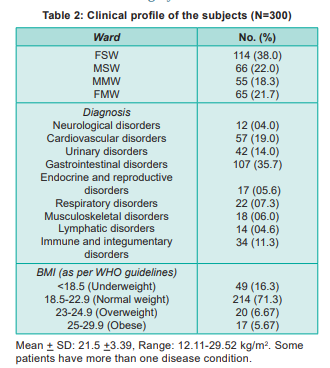
Clinical profile of subjects Table 2 depicts that 38 percent of subjects were admitted to FSW, 22 percent were admitted in MSW, 21.7 percent in FMW, and 18.3 percent to MMW. Around 36 percent of subjects had gastrointestinal system disorders, 14 percent of subjects had urinary system disorders, while 4 percent had neurological disorders. As per the WHO classification of body mass index, a maximum number of subjects (71.3%) in this study were of normal weight, 16.33 percent were underweight, 6.67 percent were overweight, and 5.67 percent were in the obese category.
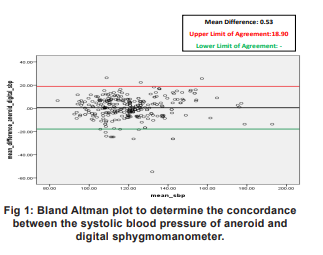
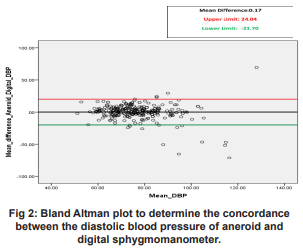
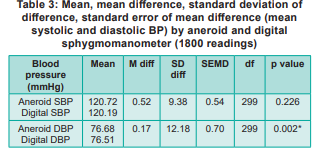
The mean SBP was 120.72 mmHg and 120.12 mmHg from aneroid and digital sphygmomanometer, respectively, with a mean difference of 0.52 (p=0.226), while the mean DBP was 76.68 mmHg and 76.52 mmHg from aneroid and digital sphygmomanometer, respectively, with a mean difference of 0.17 (p=0.002) (Table 3). Bland Altman analysis shows that the bias between systolic and diastolic blood pressure by aneroid and digital sphygmomanometer was 0.54+ 9.37 mmHg and 0.16 + 12.26 mmHg, respectively; 95.7 percent of readings in systolic blood pressure and 94.4 percent of readings in diastolic blood pressure by both devices were falling within the limits of agreement. The Bland Altman plots to determine the concordance between the systolic as well as systolic blood pressure of aneroid and digital sphygmomanometer have been shown in Fig 1 and Fig 2.
Discussion
The current research study focuses on the comparison of the effectiveness of two devices in blood pressure measurements. A total of 300 participants, i.e. patients from general wards, were taken via total enumeration. A total of six readings were recorded, three with a digital sphygmomanometer and three with an aneroid. Three consecutive readings from each device were taken at an interval of 3 minutes. A relaxation time of 10 minutes was chosen for the patients, and blood pressure measurements by another device. In the current research study, the sampling technique is total enumeration is consistent with that of Shekhar et al (2020) to measure blood pressure recordings using mercury, aneroid and digital apparatus. In the current study, the sampling technique is total enumeration, while in the study by Myers et al (2008), randomisation was used. In the current study, mean SBP was 20.72 mmHg from aneroid and digital sphygmomanometer, respectively, with a mean difference of 0.54 mmHg (p=0.226), while the mean DBP was 76.68 mmHg from aneroid and digital sphygmomanometer respectively with mean difference of 0.6 mmHg (p=0.002). Bland Altman analysis shows the bias between systolic and diastolic blood pressure by aneroid and digital sphygmomanometer as 0.54±9.37 mmHg and 0.16 ± 2.26 mmHg. According to Putripratama et al, (2015), the mean systolic blood pressure using a digital sphygmomanometer was 124.78 with a standard deviation of 24.23, and the mean diastolic was 78.22. It showed that the mean result of measurement from both devices has a significant difference, which is not consistent with the current research study. Shekhar et al (2020) studied the blood pressure recording from a conventional mercury sphygmomanometer with that from aneroid and digital devices with 102 participants, and showed that the readings are comparable and are not consistent with the current research study. Also, Ma et al (2009) evaluated the accuracy of aneroid sphygmomanometer against a mercury device, which showed no statistically significant difference for SBP and a small but significantly lower value for DBP using aneroid sphygmomanometer (Ma et al, 2015). Its result is comparable to the current research study. A study conducted by Hamied et al (2015) concluded that the digital and mercury devices can be used to replace the mercury sphygmomanometer in a community setting. (Abdul Hamied LI et al, 2015). In another study (Igbokwe et al, 2018) to assess the accuracy of aneroid and digital sphygmomanometers in the context of the mercury sphygmomanometer a total of 72 students from Nnamdi Azikiwe University, College of Health Sciences, Newi campus, Anambra State, were selected. The results showed that both instruments can be used separately for correct BP measurement. Hence, the current research study concluded that there is hardly any significant difference in the blood pressure readings measured by both of the instruments i.e. aneroid sphygmomanometer and digital sphygmomanometer.
Recommendation
A study can be replicated with a larger sample size. A study can be undertaken to compare intraarterial blood pressure with other blood pressure monitoring devices for more accuracy.
Nursing Implication
? The nurses can use digital sphygmomanometer as a means of BP measurement more frequently.
? The nurses will be able to use an aneroid and digital sphygmomanometer interchangeably.
?The nurses can plan and execute interventions effectively based on the blood pressure measurements accordingly.
Conclusion
The blood pressure readings obtained by an aneroid and digital sphygmomanometer are not significantly different, and the two devices can be used interchangeably.
1. NCI. Definition of blood pressure - NCI Dictionary of Cancer Terms - NCI. 2011 Available from: https://www.cancer.gov/ publications/dictionaries/cancer-terms/def/blood-pressure
2. Mion D, Pierin AM. How accurate are sphygmomanometers? J Hum Hypertens 1998 Apr; 12 (4): 245-48
3. Shahbabu B, Dasgupta A, Sarkar K, Sahoo SK. Which is more accurate in measuring blood pressure? A digital or an aneroid sphygmomanometer. Journal of Clinical and Diagnostic Research 2016; 10(3). Available from: (PDF) Which is More Accurate in Measuring the Blood Pressure? A Digital or an Aneroid Sphygmomanometer
4. Dasgupta PA, Pyrbot F, Paul B, Roy S, Ghosh P, Yadav A. Do the readings of digital and aneroid sphygmomanometer concur? A clinic-based study in an urban area of South Kolkata. Journal of Clinical and Diagnostic Research 2021 Aug 4; 15 (7): 18-21
5. Shekhar A, Begum S, Majgi SM. A comparative study of blood pressure recording from conventional mercury sphygmomanometer to recording from aneroid and digital device in healthy volunteers. Indian Journal of Physiological and Allied Sciences 2020; 72(1): 1-5. Available from: https:// www.ijpas.org/index.php/ijpas/article/view/30
6. Rizfan AF, Ghosh K, Mustaqir A, Mona R, Firdous J, Muhamad N. Comparison between auscultatory and oscillometric reading of blood pressure measurement while in sitting and supine position. Biomedical and Pharmacology Journal 2023 May; 12(2): 775-81. Available from:https:// biomedpharmajournal.org/vol12no2
7. Stergiou GS, Menti A, Asayama K, De La Sierra A, Wang J, Kinoshita H, et al. Accuracy of automated cuff blood pressure monitors in special populations: International Organization for Standardisation (ISO) Task Group report and call for research. J Hypertens; 2023 May 1; 41(5): 811-18
8. Myers MG, McInnis NH, Fodor GJ, Leenen FHH. Comparison between an automated and manual sphygmomanometer in a population survey. Am J Hypertens 2008 Mar; 21(3): 280-83
9. Putripratama A, Rahayuningsih S, Abdul Hamied LI, Sofiatin Y, Roesli R, et al. Mean differences between digital and mercury sphygmomanometer in community-based setting. Journal of Hypertension 2015 Jun 1; 33: e34
10. Ma Y, Temprosa M, Fowler S, Prineas R, Montez M, BrownFriday J, et al. Evaluating the accuracy of an aneroid sphygmomanometer in a clinical trial setting. American Journal of Hypertension 2009 Mar 1; 22: 263-66
11. Hamied HLI, Sofiatin Y, Rakhmilla L, Putripratama A, Roesli R. Comparison of mercury, aneroid and digital sphygmomanometer in community setting. Journal of Hypertension 2015 Jun 1; 33: e33–34
12. Igbokwe V, Ejike Daniel E, Adams M, Ikechukwu M, Atsukwei D, Rabiu K, et al. Comparative study of different blood pressure measuring instruments in humans. Advances in Biomedical Sciences 2018; 3(3): 21-29
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.